Laparoscopic Total Proctectomy with Lower Colo-Anal Anastomosis

- Laparoscopy
- Admission the day before surgery
- Bowel preparation required the day before
- Operating time 3 hours
- No nasogastric tube
- Redon drainage for 72 hours
- Provisional pouch for 1-2 months
- Drinks allowed the day after surgery
- Resumption of oral diet 2 days after surgery
- Length of hospital stay 10 days on average)
- This procedure is part of our Fast Track program (enhanced recovery after surgery [ERAS] protocol)
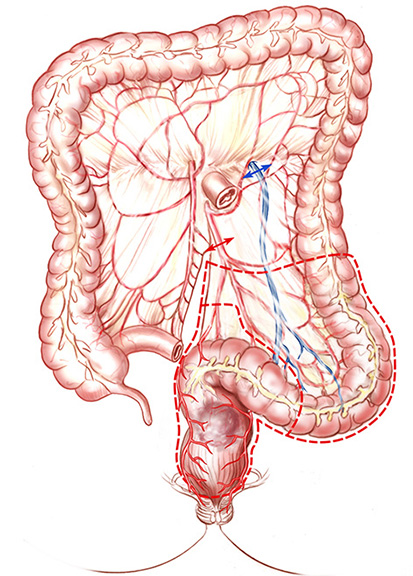
Cancers of the middle (middle third) and lower (lower third) rectum must be managed differently compared to colon and the upper rectal cancers. The preoperative assessment is the same as for tumours of the upper rectum :
- Endoscopic ultrasound performed by a specialised gastroenterologist. This test enables surgeons to evaluate the volume of the tumour and check for any suspicious lymph nodes (lymph node metastases) nearby.
- Thoraco-abdominopelvic CT scan
- Pelvic MRI also assesses the size of the tumour, its height (middle or low rectum). When the tumour develops in the lower part of the rectum, the MRI can be used to assess the degree of invasion of the anal sphincter, which plays a key role in continence.
Following these examinations, if the tumour is too large to immediately consider surgery, the surgeon will first discuss the case in a multidisciplinary concertation meeting and suggest radiotherapy associated with chemotherapy before surgery. The combination of these two treatments will reduce the volume of the tumour ("downstaging") and promote:
- Complete surgical resection of the tumour
- The most conservative possible surgery on the anal sphincter
If the anastomosis is low, the surgeon will usually be forced to create a temporary pouch (for about 2 months) to reduce the severity of a possible collapse of the anastomosis (fistula). In the case of very low tumours, near the anal sphincter, partial resection of the sphincter will be necessary. In this particular case, the realisation of a temporary pouch is not necessary. The functional result after surgery is worse than for cancers of the upper rectum because the sur-geon removes the entire rectal reservoir, meaning it is then impossible to expel stool all at once. Among men, the risk of sexual disorder is important (retrograde ejaculation, or even erectile dysfunction). For early tumours of the middle and lower rectum, the surgeon can achieve tumour resection by natural means with preservation of the rectum and anal sphincter (N.O.T.E.S). This procedure is possible in specific cases after the indication has been discus-sed and approved of in a multidisciplinary concertation meeting.
- Endoscopic ultrasound performed by a specialised gastroenterologist. This test enables surgeons to evaluate the volume of the tumour and check for any suspicious lymph nodes (lymph node metastases) nearby.
- Thoraco-abdominopelvic CT scan
- Pelvic MRI also assesses the size of the tumour, its height (middle or low rectum). When the tumour develops in the lower part of the rectum, the MRI can be used to assess the degree of invasion of the anal sphincter, which plays a key role in continence.
Following these examinations, if the tumour is too large to immediately consider surgery, the surgeon will first discuss the case in a multidisciplinary concertation meeting and suggest radiotherapy associated with chemotherapy before surgery. The combination of these two treatments will reduce the volume of the tumour ("downstaging") and promote:
- Complete surgical resection of the tumour
- The most conservative possible surgery on the anal sphincter
If the anastomosis is low, the surgeon will usually be forced to create a temporary pouch (for about 2 months) to reduce the severity of a possible collapse of the anastomosis (fistula). In the case of very low tumours, near the anal sphincter, partial resection of the sphincter will be necessary. In this particular case, the realisation of a temporary pouch is not necessary. The functional result after surgery is worse than for cancers of the upper rectum because the sur-geon removes the entire rectal reservoir, meaning it is then impossible to expel stool all at once. Among men, the risk of sexual disorder is important (retrograde ejaculation, or even erectile dysfunction). For early tumours of the middle and lower rectum, the surgeon can achieve tumour resection by natural means with preservation of the rectum and anal sphincter (N.O.T.E.S). This procedure is possible in specific cases after the indication has been discus-sed and approved of in a multidisciplinary concertation meeting.
Laparoscopic Total Proctectomy with Colo-Anal Anastomosis
- Laparoscopy
- Admission the day before surgery
- Bowel preparation required the day before
- Operating time 3 hours
- No nasogastric tube
- Redon drainage for 72 hours
- No provisional pouch
- Drinks allowed the day after surgery
- Resumption of oral diet 2 days after surgery
- Length of hospital stay 10 days on average)
- This procedure is part of our Fast Track program (enhanced recovery after surgery [ERAS] protocol)
Cancers of the middle (middle third) and lower (lower third) rectum must be managed differently compared to colon and the upper rectal cancers. The preoperative assessment is the same as for tumours of the upper rectum :
- Endoscopic ultrasound performed by a specialised gastroenterologist. This test enables surgeons to evaluate the volume of the tumour and check for any suspicious lymph nodes (lymph node metastases) nearby.
- Thoraco-abdominopelvic CT scan
- Pelvic MRI also assesses the size of the tumour, its height (middle or low rectum). When the tumour develops in the lower part of the rectum, the MRI can be used to assess the degree of invasion of the anal sphincter, which plays a key role in continence.
Following these examinations, if the tumour is too large to immediately consider surgery, the surgeon will first discuss the case in a multidisciplinary concertation meeting and suggest radiotherapy associated with chemotherapy before surgery. The combination of these two treatments will reduce the volume of the tumour ("downstaging") and promote:
- Complete surgical resection of the tumour
- The most conservative possible surgery on the anal sphincter
If the anastomosis is low, the surgeon will usually be forced to create a temporary pouch (for about 2 months) to reduce the severity of a possible collapse of the anastomosis (fistula). In the case of very low tumours, near the anal sphincter, partial resection of the sphincter will be necessary. In this particular case, the realisation of a temporary pouch is not necessary. The functional result after surgery is worse than for cancers of the upper rectum because the sur-geon removes the entire rectal reservoir, meaning it is then impossible to expel stool all at once. Among men, the risk of sexual disorder is important (retrograde ejaculation, or even erectile dysfunction). For early tumours of the middle and lower rectum, the surgeon can achieve tumour resection by natural means with preservation of the rectum and anal sphincter (N.O.T.E.S). This procedure is possible in specific cases after the indication has been discus-sed and approved of in a multidisciplinary concertation meeting.
Transanal Resection (N.O.T.E.S.)
- For early-stage cancer
- Tumour resection through natural orifice
- Admission the day before surgery
- Bowel preparation required the day before
- Operating time 1 hour
- No nasogastric tube
- No provisional pouch
- Drinks allowed the evening after surgery
- Resumption of oral diet the day after surgery
- Length of hospital stay 2 days on average
- This procedure is part of our Fast Track program (enhanced recovery after surgery [ERAS] protocol